
Introduction
Atopic eczema is one of the commonest diseases of dermatology
Large majority of patients who get it will develop symptoms or signs by the age of 5
Prevalence:
In UK:
≈ 25% (15-44%) < 5yo
≈ 5-10% of adults
Higher prevalence in Australasia and Northern Europe compared to the rest of Europe and Asia
Severity of disease tends to get better with age but patients still may carry a presdisposition to it and have increased sensitvity to things in the environment like irritants and allergens
This is important to remember as it may predispose them to occupational skin disease (eg hair dressers, health care workers)
Associations:
Prior studies:
≈ 25% develop asthma
≈ 75% develop allergic rhinitis
(Although recent studies may suggest above associations may not be this high)
Food allergies
More prone to skin infections due to reduced cellular immunity found in this condition. Patients more prone to develop bacterial, fungal and viral infections (eg herpes simplex)
Hygiene hypothesis:
Eczema is positively associated with -
Being from a small family
Living in urban area compared to rural area
Atopic eczema prevalence has increased x 2-3 fold over the last 30 years giving rise to the ‘hygiene hypothesis’ to account for the increased prevalence:
In a a nutshell: ‘The cleaner the environment you grow up in, the more likely you are to have eczema’
Early exposure to microbes and their products may help steer the immune system away from atopic dermatitis and allergic disease
Therefore less exposure to allergens/infections early in life can lead to increased incidence of autoimmune and allergic diseases
Things like early exposure to older siblings, children going to creche and having a pet like your own dog may protect agaisnt atopy
‘Atopic march’
Refers to the natural history of atopic manifestations
Initially young atopic patients present with eczema and food allergies
These then become less common with age
Later asthma occurs and also with time this becomes less common
In adults most likely will have allergic rhinitis
Literature supports a causal link between AD and later-onset atopic disease (the "atopic march")
A dysfunctional skin barrier allows allergen entry via the skin rather than the gut — an abnormal route of exposure, e.g. in food allergy
This drives epicutaneous sensitization to those allergens
Which induces abnormal systemic immunity, predisposing to allergic rhinitis, asthma, and even food allergy
Clincal presentation
Is a clinical diagnosis
Investigations usually not needed
Patients often have dry skin with a red, scaly rash
Is an itchy condition
Patients can often have secondary changes such as scratch marks and excoriations
With chronicity and scratching skin can become thickened with lichenification (exaggerated skin margins)
If skin becomes weepy or crusted it is often a sign of secondary infection
Skin can become dyspigmented (hyper or hypo) particularly in darker skin types
There are UK diagnostic criteria (in my experience, rarely used day-to-day, as most clinicians diagnose AD on overall clinical impression rather than formal criteria):
Itchy skin condition plus ≥3 of:
Itchy flexural rash (or rash on cheeks if <4y)
History of asthma or rhinitis (or history of atopy in a 1st-degree relative if <4y)
General dry skin in the past year
Visible flexural eczema (or cheeks/forehead/outer limbs if <4y)
Onset in the first 2 years of life
Patterns of eczema with age:
1/Infantile phase (0-6 months)
Seborrhoeic dermatitis (cradle cap)
Usually appears on face: cheeks, chin and forehead
But can spread elsewhere
The diaper area is usually not affected (moisture protects the skin)
The skin can look red and weepy
2/ Babies (6-12 months)
Rash often appears on extensors of elbows and knees (places that are easy to scratch as they crawl)
3/ Childhood phase (2-10 years)
Often develop a mainly flexural presentation: elbows, knees, wrists, ankles and neck
Can also affect peri-oral and peri-orbital areas
With chronic rubbing of skin can get lichenification (thick skin with exaggerated skin markings. Lichenification usually a bigger problem in darker skin types)
Oozing and crusting with secondary infection can occur
With chronic rubbing of skin can get lichenification (thick skin with exaggerated skin markings. Lichenification usually a bigger problem in darker skin types)
Lichenification (courtesy Dr. McColl)

Adolescent phase (12-20) to adult phase (>20)
Atopic dermatitis often improves although barrier function is always decreased
Flexural eczema may still be present and eczema may be characterised by thick lichenified plaques from scratching
With severe eczema can get prurigo nodules as a reaction to chronic rubbing. These appear as nodules.
These can be extremely itchy and need strong topical steroid to penetrate this thick skin
Patients often start to develop more localised eczema (eg hand dermatitis or peri-ocular dermatitis) which may also be irritant or allergic (see contact dermatitis section for more info on this)
Hand dermatitis

Clues to diagnosis of atopy:
Atopic patients may have ichthyosis vulgaris (due to filaggrin mutatoin - discussed later) so may also have:
Hyper-linear palms of hands
Keratosis pilaris
Sub-types of eczema:
Discoid eczema:
Common type of eczema that can occur in atopic eczema
Get scattered, roundish patches of eczema that can be intensely itchy
Often need a potent topical steroid to get discoid eczema under control
Discoid eczema
Pityriasis alba:
Common manifestation of atopic eczema in younger people
Especially in darker skin type
Hypopigmented scaly areas seen: often on face but also on back and thighs (may be mistaken for pityriasis versicolor or even vitiligo)

Pityriasis alba
Nodular prurigo:
With chronic rubbing and scratching can get thickened, intensely itchy, hyperkeratotic nodules — typically on the extensor arms and legs — which tend to persist and become self-perpetuating

Infection
Having atopic skin puts you at increased risk of infection (including bacterial, viral, fungal and molluscum infection)
Bacterial infection:
If skin is particularly weepy or see honeycomb crusting think bacterial infection
Atopic dermatitis patients tend to be colonised with staph aureus (30-100%)
Colonisation increases the risk of infection
MRSA:
11-34% of AD patients colonised with S aureus have MRSA
MRSA associated with more severe eczema
If have an eczema patient who is very resistant to treatment you should consider swabbing skin to make sure they don’t have MRSA
MRSA carriage eradication example (but should look up local guidelines):
1/Mupirocin in nares tds for five consecutive days
2/An appropriate wash (eg octenisan) daily x 7 days
For more on microbiome and MRSA infection click on link
PVL (Panton valentine leuckocidin) staph aureus:
PVL is a toxin produced by certain types of S aureus
The toxin can kill white blood cells and cause damage to skin and deeper tissues
Clinically it can present with cellulitis, abscesses, boils and folliculitis so suspect in eczema patient who is getting recurrent boils
More about PVL at end of atopic eczema section
Streptococcal infection eczema:
Can also get Grp A streptococcal infection in atopic dermatitis patients
May see pustules with streptococcal infection and can be painful
Eczema herpeticum:
Dermatological emergency
Occurs when atopic eczema becomes secondarily infected by herpes virus
Suspect if get sudden flare up of eczema and child is unwell (fever, lymphadenopathy etc)
Look for small blisters and classical ‘punched out erosions’
If it is around the eye needs urgent ophthalmology review to outrule eye involvement
Important to recognise early and to put patient on oral or IV antivirals
[for dosing look at BNF and treat as for immunosuppressed patient as skin is ‘locally immunosuppressed’ in eczema]
Can use acyclovir
Valciclovir actually shows better bioavailability and can be more effective but it is more expensive
Often becomes secondarily infected with bacteria so look for crusting and treat with antibiotics
Infection in atopic skin with coxsackie virus (eczema cocksackium) and chickenpox can cause similar clinical picture

Pathogenesis
A complex range of factors at play:
Skin barrier dysfunction
Immune dysregulation
Environmental factors (allergens, altered skin microbiome)
Genetics
Their relative roles and whether they are all inter-related is still not fully understood
As it is so complex I will go through simplified versions but which will hopefully give a better understanding of the various current therapeutic approaches
Ways to conceptualise it:
Primary problem is a barrier defect which leads to immune dysregulation (outside in theory)
Primary problems is immune dysregulation which leads to the barrier defect (inside out theory)
Eczema as a barrier defect:
Keratinocytes in skin start out at basal layer and during life cycle work there way to the surface
At the surface they become flattened and are known as corneocytes
This outermost layer of the epidermis is called the stratum corneum
The stratum coreum provides the majority of the barrier function of skin
Think of the stratum corneum as a brick wall
The corneocytes are analogous to bricks
The lipid lamellae are analogous to cement
In eczema you have a barrier defect:
Therefore can’t keep water in skin as efficiently which can lead to dysfunction of the skin
Things from the environment get in to the skin like air pollutants, bacteria, irritants and allergens
These are presented to the dendritic cells of the immune system
These activated dendritic cells promote a shift from Th1 cell activity to Th2 cell activity
Increase Th2 cell activity leads to an increase in its signature cytokines such as IL 4 IL 13 and IL 31
[IL-31 is a cytokine that produces itching]
With increased inflammation the patient itches and then scratches
This further disrupts the barrier and allows more antigens/bacteria in creating an itch-scratch cycle that makes the eczema worse
Th2 cytokines also:
Downregulate important proteins in skin (eg filaggrin)
Facilitate transcutaneous sensitisation
Facilitate bacterial binding and infection
This is a simplified version of the eczema pathway which involves environtmental factors further degrading the barrier, chemicals released from keratinocyts (eg TSLP), eosinophils and increased production of IgE
Genetic factors:
Genetic factors and skin barrier dysfunction:
Multiple genetic factors have been identified that can lead to a defect in the skin barrier
Mutations in filaggrin are the most well documented (at least 20 loss of function causing filaggrin deficiency have been identified)
Lack of this protein in the skin causes an inherited dry skin condition called ichtyosis vulgaris and is strongly linked to development of atopic eczema
Filaggrin is vital for skin cells to mature properly into the tough, flat corneocytes that form part of the stratum corneum
Filaggrin is formed from the breakdown of profilaggrin which is a protein contained in the granules of the granular layer of the epidermis
After cleavage, liberated filaggrin binds to and collapses the keratin cytoskeleton, resulting in flattened keratin cells aligned parallel to the outer surface of the epidermis. This improves barrier function.
Therefore without filaggrin the keratinocytes are not aligned properly and antigens can easily enter and meet antigen presenting cells causing an immune response
With fillagrin intact
Filaggrin not functioning
Also, when filaggrin is degraded its degradation products are important in:
1/retaining moisture (natural mositurising factor)
2/killing bacteria
3/maintaining skin pH
Therefore not having enough filaggrin leads to impaired barrier function, inability to retain water, dry skin, abnormal pH and too much bacteria .
Filaggrin mutations are associated with:
Increased risk of atopic eczema
Increased risk of allergic sensitisation
Increased risk of peanut allergy
But not all cases of eczema are related to filaggrin issues:
70-80% of eczema cases worldwide have no filaggrin mutations
(FLG mutations found in 18% British cohorts)
Other genetic candidates are being explored which can cause impaired barrier function by causing:
Increased proteases in skin
Decreased protease inhibitors
Problems with adhesion proteins between corneocytes
Severity assessment
It is good to assess how much the eczema is affecting the patient
Should ask aout sleep disturbance, missed days of school/work
Quality of life questionnaires:
DLQI (how it affects your quality of life over the last weeks: scored out of 30)
POEM (Patient oreientated eczema measure - more specific to eczema. Again how it affects QoL over the last week. Scored out of 28)
Clinical severity assessment scores:
EASI
Looks at 4 body regions (head/neck, trunk, upper limbs, lower limbs)
Assesses the area affected in each region
Looks at redness, thickness (induration, papulation, oedema), scratching (excoriations) and licenification
Get combined score much like PASI
SCORAD is another severity assessment score sometimes used
Management
General:
Very important to take time particularly in the first consultation to counsel on what eczema is and why you use topical treatments
When counselling patients or parents can use the analogy of a house made with brick walls
The emollient is very important in keeping the brick walls well maintained and in good condition
However if the house catches on fire (skin is red) then topical steroids (or other anti-inflammatories) will be needed to put this fire out
Cleansing
Soaps, shower gels, shampoos and baby bubble baths are very irritant and should be avoided
Soap substitute or emollient bath additive should be used instead. Can also use these to wash hair.
Fragrances and perfumes are also known irritants to skin and should not be used.
When bathing child- only use bath for 5-10 minutes. As soon as finished pat (instead of rubbing) down child with towel. Then use a greasy ointment such as emulsifying ointment as soon as they are out and this will lock in the moisturiser (‘soak and seal’)
Examples of soap substitutes
Dermol 500, QV gentle wash, hydromoll bath and shower, doublebase emollient wash gel
Bath additives examples:
Oilatum junior bath additive, doublebase bath additive, hydromol emollient bath additive, E45 emollient bath oil
Emollients
Hydration is key in dealing with atopic patients
Use as much emollient as possible
When estimating how much emollient is enough to prescribe:
The average needed for 2 applications daily for 1 week is:
500g in adults
250g in children
When using emollients we ask parent to use a clean spoon when taking it out of the tub as if use hands when taking out emollients it may introduce bacteria into the tub
The greasier an emollient is the better it will hydrate the skin (eg Hydromoll ointment)
But it is often about finding the best emollient that parents will actually adhere to using as some parent find some ointments are far too greasy and stick on clothes
Ointments- have less ingredients so child less likely to react/develop allergy to an ointment. Therefore they are generally preferable to creams but they can be very greasy so sometimes as child gets older become less practical.
Creams- contain emulsifiers, preservatives and antimicrobials and may sting more than ointments.
Common emollients used in UK:
Ointments: Hydromol ointment, Epaderm ointment, Diprobase ointment, QV ointment, Cetraben ointment
Emulsifying ointment tends to be used in Ireland
Creams: Aveeno cream, diprobase cream, cetraben cream
Silcocks base tends to be used in Ireland
From light consistency to greasy consistency:
Aveeno, Zeroveen, Balneum, Doublebase gel
Zerobase
Cetraben cream
Emollin spray (50:50 spray)
Cetraben ointment
Zeroderm ointment
Hydromoll ointment
50:50 ointment
Parents often ask if child can go swimming.
In general it is okay to use swimming pools.
Tips would be to mositurise the baby before swimming.
Use a whole body swim suit as otherwise baby (helps with grip as otherwise baby would be slippy)
As soon as baby is out use a soap substitute if possible (to wash off the chlorine which can be irritating) and then moisturise afterwards
Topical corticosteroids
Extremely important in managing eczema
Often times parents have steroid phobia but if used correctly are very safe
Important to use appropriate strength of steroids depending on location of the rash and patients age
In general use weaker steroids in areas of thin skin (face and eyelids) and can use stronger steroids in areas of thick skin (palms and soles of feet) with skin on the body somewhere in between
Steroid potencies (commonly used bold)
Weak: Hydrocortisone 1%
Moderate: Eumovate (clobetasone butyrate), Betnovate rd (1/4 strength betnovate), Haelan tape (fludroxycortide)
Potent: Betnovate (betamethasone 0.1%), Elocon (mometasone), Synalar (fluocinolone)
Super potent: Dermovate (clobetasol propionate)
Combination topicals:
Fucidin H: hydrocortisone and fucidin (weak steroid, antibacterial)
Daktacort: hydrocortisone and clotrimazole (weak steroid, antifungal)
Betnovate C: betamethasone valerate and cliquinol (antibacterial): generally preferable to fucibet as resistance to fucidin is common
Fucibet: betamethasone valerate and fucidin (strong steroid, antibacterial)
Trimovate: Eumovate/neomycin/oxytetracycline (moderate steroid, anti-fungal, anti-bacterial)
Lotriderm: Betamethasone diproproionate and clotrimazole (strong steroid, anti-fungal)
Dermovate NN: Dermovate, neomycin, nystatin (super-potent steroid, anti-bacterial, anti-fungal)
Generally ointments are preferable to creams as there is less preservatives in them.
Steroids should work quickly, if child is not responding within a week then you might not be using enough steroids, steroid is not strong enough, or something else is wrong
One potential routine:
Many potential routines for topical steroid use exist, here is one such example:
When a flare is present: often give the appropriate steroid daily for 7-10 days (no major benefit from using twice daily with single steroid preparations)
Then when it is under control use it twice weekly as maintenance (using it twice weekly won’t cause any long term effects)
Finger tip units
Finger tip units are a useful measure of how much steroid is needed to cover particular body parts
1 FTU is encough to treat an areas of skin twice the size of the flat of and adult’s hand with fingers together
In general:
Head to toe treatment for adults is 20-30g so daily treatment for 1 week 140g
Child 6-12 months: 5g so daily treatment 1 week is 35g
Child 4 years: 6g so daily treatment 1 week 42g
Child 6-10 years: 8g so daily treatment 1 week 56g
Topical calcineurin inhibitors (TCI)
Often used as steroid sparing agents
Particularly good for face and flexures
Might initially burn and sting but tends to get better with continued use
Should start using when skin not too badly inflammed to prevent stinging (so might want to give topical steroid for few days initially to get flare under control)
Pimecrolimus (elidel)- 1/3 as potent as tacrolimus
Tacrolimus (protopic)- comes in two strengths
0.03% licensed > 2 years
0.1% licensed > 16 years
(Stronger strength often used off license in younger age groups in dermatology)
Can do different routines for example:
Acute flares twice daily for 3-4 weeks
Maintenance: twice weekly up to 1 year (appears to reduce number of eczema flaress)
Or other types of routine such as topical steroid x 1 month, then protopic x 1 month
Side effects:
Increased HSV has been reported so ask them to stop if develop cold sores but in general in practice doesn’t appear to be major issue
Theoretical risk of increased risk of skin cancer as is an immunosupressant but this doesn’t seem to be the case after decades of clinical practice (black box warning so may want to warn patients about this in advance so they are not alarmed)
[APPLES study: no evidence found that topical tacrolimus increases long-term cancer risk in children with AD after 10 years follow up
Children must of used tacrolimus for 6 weeks]
Novel topical agents
Ruloxitinib
JAKi
Recent phase 2 study shows superior to mid-strength steroids (Kin et all 200, JAACI)
Increasing strength of of ruloxitnib get increasing response in EASI scores
Some reports here of 80% improvement in EASI in sites used
True AD-1 and True AD-2 studies sample 1250 patients and in essence replicated the above study
Delgocitinib:
Occlusion and garments
Occlusion can be beneficial by improving hydration, steroid penetration, acting as a barrier to scratching and improving sleep
Methods:
Paste bandages
Wet wraps
Garments
Occlusive dressings
Good education is needed on the use of occlusion
The BAD website: skinhealthinfo.org.uk has good informational videos on how to apply occlusive dressings, paste bandages and wet wraps (supports and resources: video guides)
Occlusion cautions:
Increases potency of steroid used so use steroids in appropriate areas (not face, flexures)
Can exacerbate active skin infection
Paste bandages:
Single use only
Icthopaste (6.32% zinc oxide), Viscopaste (10% zinc oxide), Zipzoc bandages (20% zinc oxide)
Icthopaste and viscopaste are cotton wrap around bandages
Zipzocs are cotton stockings (often easier to apply than wrap around bandages above but children are too small to use them)
They have soothing and anti-inflammatory pathways and can improve penetration of topical steroids due to occlusion
You need to cover bandages and stocking with a tubular dressing to avoid soiling of clothes and to help keep them in place
A tip is to put the paste bandages in the fridge before application which can be soothing
Products can be left in place for seven days if indicated but obviously often changed more frequently depending on need for emollient and topical steroid
Wet wraps:
Most commonly used with emollient underneath but can be used with topical steroids underneath for short periods of time
When applying will need garments: 2 tops, 2 leggings, warm water and emollient cream (to cover smaller areas can use tubular bandaging instead)
After washing you apply a thick layer of cream
Wraps are prepared by putting 1 top and 1 leggings in a bowl of warm water, then squeezing garments of excess water so they are damp but not dripping wet
They are then applied to the patient (make sure labels/seam are on the outside) and then put dry top and leggings on top
Can be left on for 24 hours but often are left on overnight and taken off in the morning
Caution:
If think have skin infection do not use them as can make them worse
Can be uncomfortable for patients particularly in cold weathere
Eczema garments:
Are sometimes referred to as ‘eczema clothing’
They are desinged for individuals with eczema and other similar conditions
They aim to reduce itching and prevent scratching
For babies they may include mittens and footies and may have a head garment
Types of garments from cheapest to most expensive:
Clinifast (viscose)
Skinnes (viscose)
Skinnies (silk)
Dreamskin
Occlusive dressings:
Hydrocolloid dressings that are applied over treatment to improve absorption of the medication and prevent damage from scratching
It increases the strength of the steroid so should be used only for a short period of time and should not be used if the skin is affected
Avoid occlusive dressings on face or flexural areas
An example of an occlusive dressing that can be used is duoderm extrathin
Bleach baths
Can be used with the proposed aim to reduce bacterial load (eg S Aureus) and as such to reduce Eczema severity so may consider if patients get recurrent secondary skin infections
How to use:
Use pure bleach without fragrance or soap
Examples:
Tesco everyday value thin bleach
Milton disinfecting solution
ASDA Smart Price thin bleach
Run bath with no additives:
Add half a cup (150ml) of bleach to at least 10cm depth of water in an adult bath
(For baby tub use 2ml bleach for each 1L water)
Mix well
Soak for 10-15 minutes
Can use an emollient cream to clean skin when soaking
Can wet face and hair (should not cause harm if gets in eyes or mouth) but make sure child is not drinking it
Then rinse with plain water, pat skin dry and apply emollients as usual
Use once or twice a week
Telling parents to use a bleach bath can sometimes alarm them so can use the analogy that it essentially is like ‘making your own swimming pool‘
Phototherapy
Narrowband UVB:
Time consuming but can be useful for management of eczema
Not as effective as for psoriasis and may need longer treatments
Important to emphasize frequent moisturising as it is good for inflammation but the skin can dry out
Antihistamines
Don’t really work well for itch of eczema!!!
Occasionally sedating anti histamines can be used if patient not sleeping but should only prescribe very short course of this
Conventional systemic agents
In general Methotrexate is the main workhorse and we use Ciclosporin in certain circumstances (eg when need rapid relief or for pregnant patients)
Azathioprine and Mycophenolate mofetil are other options but are very rarely used these days due to the advent of new biologic agents
Azathioprine appears to have similar efficacy to methotrexate but has a worse side effect profile (increased risk of skin cancers and haematological malignancies with long term use)
In general should try to avoid oral steroids in atopic eczema. May work at the start but when they are stopped may get worsening flare of condition.
The TREAT trial:
Surprisingly, there was a lack of randomised controlled trials directly comparing methotrexate and ciclosporin in the treatment of eczema until 2023 — TREAT (Flohr et al.) is the head-to-head that finally filled that gap.
Methdology:
Design: Multi-centred RCT
Population: Looked at paediatric population with severe atopic dermatitis
Comparison: Methotrexate 0.4 mg/kg/week vs ciclosporin 4 mg/kg/day
Duration: 36 weeks of active treatment + 60 weeks of follow-up — the long follow-up is what lets it capture what happens after stopping (durability vs rebound)
Take-homes:
Ciclosporin is faster — better early response, wins out to ~20 weeks.
MTX catches up, then overtakes — from week 20 onwards methotrexate is the more effective drug.
MTX is more durable — less flaring after stopping; ciclosporin rebounds.
Test dose for methotrextate deemed unncecessary — TREAT used one, but the safety data supported starting at the therapeutic dose with reassuring baseline bloods.
Both drugs were well tolerated and safe in the trial.
Think of methotrexate as the tortoise, and ciclosporin as the hare

Methotrexate dosing:
Once-weekly methotrexate, on one chosen day each week
Adults
- Start 15 mg once weekly, then titrate to max 25 mg/week
- Start lower / consider a test dose in the elderly, multiple co-morbidities, or renal impairment
Folic acid
- 5 mg once daily, on every day except the methotrexate day
Children
- 0.2–0.7 mg/kg once weekly (max 25 mg/week)
- Weight-based; one day each week only
Folic acid
- 1 mg once daily, on every day except the methotrexate day
- Or 5–6 mg once weekly, on a different day to methotrexate
Switching to subcutaneous
- Consider subcutaneous methotrexate if oral response is inadequate, or if there are symptoms of nausea or other GI upset
- Better and more predictable bioavailability
Ciclosporin:
Dosing
3–5 mg/kg/day, divided twice daily
Use ideal body weight (can look up on www.mdcalc.com) rather than actual weight in significantly overweight patients
Once controlled, taper down in steps to the lowest effective dose, rather than stopping abruptly.
Duration
Think of it as a short-course rescue drug, not a maintenance option. Generally do not want to be giving it for longer than around 1 year of continuous use.
Expect a response within 2–6 weeks — it's the fastest of the conventional systemics.
The limiting factors are nephrotoxicity and hypertension, both cumulative, which is why the duration is capped.
Rebound is common on stopping, so plan the exit before you start — either a taper, a handover to methotrexate, or a switch to a biologic/JAKi.
In practice: use ciclosporin to get someone out of crisis (sleep destroyed, missing school or work), and use that window to establish a more durable option.
Biologic medications
Generally we need to try one conventional systemic agent (eg methotrexate) prior to moving on to the biologic therapies
The targets at a glance:
IL-4 / IL-13 → Dupilumab
IL-13 → Tralokinumab, Lebrikizumab
IL-31 receptor → Nemolizumab (the "itch" biologic)
Dupilumab
Dupilumab was the first targeted biologic approved for atopic eczema.
Fully human monoclonal antibody to an IL-4 receptor subunit (IL-4Rα)
Both IL-4 and IL-13 bind to receptors that contain this subunit
IL-4 and IL-13 are both Th2 cytokines increased in eczematous skin
Increased IL-4 and IL-13:
Impairs keratinocyte differentiation
Lower anti-microbial peptide production
Increases eosinophil recruitment
Causes further TH2 differentiation and survival
Dupilumab — efficacy
LIBERTY AD OLE is the long-term extension, running up to five years, with response maintained rather than lost over time.
EU approval:
Dupilumab is approved from 6 months of age in patients who are candidates for systemic therapy (‘severe’ disease under 12 years; ‘moderate-to-severe’ from 12 years)
Indication:
Moderate to severe eczema who have failed at least 1 systemic agent.
Also licensed for nodular prurigo
Other (non-derm) indications (include but not limited to):
Chronic rhinosinusitis with nasal polyposis
Severe asthma.
Note: If a patient is on dupilumab for eczema and also has asthma, warn them the asthma may rebound if dupilumab is stopped.
Dosing in eczema:
Adults: 600 mg subcut induction, then 300 mg every 2 weeks (weight > 50 kg)
Adolescents (12–18) / adults < 50 kg: 400 mg induction, then 200 mg every 2 weeks
Review at 16 weeks — continue if adequate response (≥50% reduction in EASI or 4-point drop in DLQI).
Not considered strongly immunosuppressant (no meaningful increase in TB or opportunistic infection).
Screening and monitoring
In practice, many centres still perform a baseline biologic screen before starting
Many continue annual bloods while patients remain on treatment, largely by local protocol carried over from other biologics.
Other units are moving away from routine monitoring altogether.
The 2023 AAD guidelines are explicit that no laboratory monitoring is required either before initiation or during treatment, reflecting that dupilumab is immunomodulatory rather than immunosuppressive with no myelosuppression, hepatotoxicity or reactivation risk to monitor for.
Davis DMR. J Am Acad Dermatol 2024;90(2):e43–e56 — https://www.jaad.org/article/S0190-9622(23)02878-5/fulltext
Side effects
Dupilumab related ocular surface disease (DROSD)
Approximately 25% (5-42%) develop DROSD within the first 4 months of treatment
Roughly 4% of patients stop dupilumab because of eye problems in real-world cohorts, but withdrawal is thought to be genuinely necessary in only about 0.5% — the gap underlines that most DROSD can be controlled without stopping treatment.
Recent BAD / Royal College of Ophthalmologists consensus guidelines (Ardern-Jons et al. BR J Dermatol 2024) offer a clear approach to grading severity and managing it — usually without stopping dupilumab.
Step 1: Exclude red flags first
RAPID red flags — urgent (within 24 h)
Redness must be present, plus any of:
- A — Acuity loss (worsening vision)
- P — Pain (true ocular pain, new onset — more than grittiness)
- I — Intolerance of light (photophobia)
- D — Damaged cornea (ulceration, haze, opacity or purulent discharge)
Redness + any one flag (score ≥2), OR any unilateral red eye → ophthalmology within 24 h.
Step 2: Grade severity
Mild
Mild redness
Mild itch / irritation. No discharge.
Moderate
Moderate redness
More marked irritation. No discharge.
Severe
Severe redness
Marked irritation with clear discharge.
Grade on the most severe feature — redness and symptoms do not always correlate (Efron grading).
Children < 7: ocular symptoms warrants early ophthalmology advice as young children can tolerate significant inflammation and report symptoms poorly. Significant inflammation can also interfere with neuro-ocular development.
Step 3: Treatment Dermatology led
First-line
Preservative-free lubricants (e.g. hypromellose or sodium hyaluronate), 3–4 times daily.
Second-line
Add a topical antihistamine eyedrop (olopatadine) twice daily if lubricants alone are ineffective.
Third-line (moderate-to-severe)
Tacrolimus 0.1% ointment to the lid margins once daily for 4 weeks. In 7–17 year-olds, only after ophthalmology advice; arrange ophthalmology review within 4 weeks once tacrolimus is started.
Step 4: Not responding?
Mild → routine ophthalmology referral;
Moderate-to-severe (or anyone on lid-margin tacrolimus) → refer within 4 weeks.
Ophthalmology may add:
A short course of topical corticosteroid (max ~8 weeks), ciclosporin eye drops (steroid-sparing), or autologous serum drops in refractory cases.
For refractory or troublesome DROSD, consider extending the dupilumab dosing interval, or switching to a therapy less associated with ocular disease — such as a JAK inhibitor (DROSD often resolves) or tralokinumab.
Multicentre retrospective study (RESO-ADOC study) - Beyrouti et al., 2025, J Allergy Clin Immunol Practice
Examined 106 patients with atopic dermatitis who discontinued dupilumab because of ocular adverse events and/or facial redness, then switched to either tralokinumab or a Janus kinase inhibitor, with outcomes assessed 3–6 months after the switch.
For the ocular disease specifically, it resolved or improved in ~72% (tralokinumab) vs ~92% (JAKi) at 3–6 months — though this counts anything from full resolution to partial benefit, and stopping dupilumab itself likely contributes.
Dupilumab facial redness (DFR)
aka Dupilumab-associated head & neck dermatitis (DAHND)
A subset of patients on dupilumab develop a new rash on the face and neck while the rest of their skin clears.
This is likely a distinct entity though in practice it can be hard to separate cleanly from a patient's own facial eczema.
It affects roughly 4–10% of patients
The erythema usually develops within 2 months of initiating treatment but can also appear as late as 9 months after starting therapy
Clinical picture
Well-demarcated erythematous patches in a seborrheic distribution — central face, nose and brows, hairline and neck — with scaling, desquamation and a burning quality rather than itch.
In skin of colour the redness takes on violaceous or dusky tones and may be harder to pick up
Why it happens
Dupilumab blocks IL-4 and IL-13, the core "Th2" signals driving atopic dermatitis. The switching off this pathway lets a different inflammation surface on the face. Two candidates lead.
Malassezia hypersensitivity:
By blocking the Th2 pathway to treat eczema, dupilumab inadvertently skews the immune system toward a Th17-driven inflammatory response.
This altered immune environment causes the skin to become hypersensitive to Malassezia and cause a rash in a seborrhoeic distribution
Elevated pretreamtent Malassezia specific IgE can be associated with this condition
A "type 22" immune switch (the newer model):
Bangert et al,(Nat Commun 2024) demonstrated that as the IL-4/IL-13 markers settle it causes a type 22 immune response with an increase in the cytokine IL-22. This cytokine stimulates keratinocytes causing inflammation and erythema
Other explanations have been proposed too — a rosacea-like reaction, a sebopsoriasis-like picture, and unmasked allergic contact dermatitis (worth patch testing first)
DAHND versus eczema
It's worth trying to distinguish DAHND from facial eczema that is simply flaring, or responding less completely than the rest of the body — the head and neck are known to clear less well on dupilumab than other sites.
So a key question is: hastheir facial eczema always looked like, or is it behaving differently?
That distinction isn't always possible, though: In one systematic review, roughly half of these patients had pre-existing facial or neck AD, while the other half described symptoms unlike their usual eczema.
Jo et al, 2021, JAAD: https://www.jaad.org/article/S0190-9622(21)00079-7/abstract
Management
Topicals are the mainstay — protopic with short pulses of a low-potency steroid (e.g. hydrocortisone 1% or clobetasone/Eumovate) for flares.
If that's not enough, consider stretching the dupilumab dosing interval (e.g. every 3–4 weeks rather than fortnightly).
For persistent cases, switching is the next step — the best evidence is for JAK inhibitors (upadacitinib, abrocitinib), which often clear DAHND within weeks, with tralokinumab as an option if a JAKi is inappropriate
In the Beyrouti trial previously mentioned - resolution or improvement of facial redness was achieved in 85% of those switched to a JAK inhibitor versus only 33% of those switched to tralokinumab
Dupilumab associated inflammatory arthritis (DAIA)
A small group of patients develop new joint pain, enthesitis or tenosynovitis on dupilumab, often while the skin is doing well.
Pooled prevalence in a 2025 meta-analysis was 2.62% (95% CI 1.44–4.70), and onset is usually within four months of starting, though it can occur after the first injection or much later.
Tow Hx et al, Dermatitis, 2025: https://pubmed.ncbi.nlm.nih.gov/40435582/
Clinical picture
Symptoms are usually peripheral, generalised and symmetric, and onset is typically within four months of starting dupilumab — though it can range from immediately after the first injection to many months in.
Some patients report a clear relationship to injection timing. Symptoms and signs:
Enthesitis - achilles tendon, lateral epicondyle, patellar tendon
Dactylitis
Inflammatory back pain place it within the spondyloarthritis spectrum
It is characteristically seronegative — RF and anti-CCP negative, inflammatory markers often normal — so a normal screen doesn't exclude it.
Ultrasound or MRI may show enthesitis.
Management:
Management is by severity.
Mild — continue dupilumab with as-needed NSAIDs.
Moderate — prescription NSAIDs, consider stretching the dosing interval, refer to rheumatology.
Severe — stop dupilumab; most resolve fully within weeks, and switching to a JAK inhibitor covers both joints and skin
Phenotypic switching
A small number of patients on dupilumab develop psoriasis or psoriasiform plaques where they previously had eczema.
The mechanism is familiar: blocking IL-4/IL-13 removes the brake on the Th17 axis, and psoriasis-type inflammation surfaces
Think of it when a patient develops well-demarcated scaly plaques on scalp or extensors rather than a typical eczema flare, and biopsy rather than assuming refractory disease.
The eruption usually settles on stopping dupilumab, but the eczema can rebound
Other side effects
Infection:
Perhaps slight increased risk of eye infections, oral herpes and increased risk of parastitic infections (due to decrease in eosinophils)
However dupilumab does not appear to increase infection risk significantly.
Overall rates match placebo, and serious infections, bacterial skin infections and eczema herpeticum are all less frequent, most likely reflecting restored barrier function as the eczema clears.
Eosinophilia - usually transient and self limited
Flare of asthma on stopping the drug
Blood screening and monitoring:
Potential protocol:
Document prior treatments
Record baseline DLQI, POEM, EASI
Routine bloods and pre-immunosuppression screen (no need for CXR/Quantiferon)
Contraception for females (can’t know for sure it is safe in pregnancy. Has 11-week washout period)
Consider prophylactic hyloforte (lubricating) eye drops four times a day for 2 weeks prior to starting treatment (can increase to 8 times/day if symptomatic)
Potential monitoring:
Review at 8-weeks: enquire about eye symptoms, ? facial worsening, initial efficacy
Review at 16-weeks: Routine bloods, DLQI, EASI, POEM and decide whether to continue
Review 6 monthly thereafter: routine bloods, DLQI, EASI, POEM
Tralokinumab
Monoclonal antibody binding the IL-13 cytokine itself, rather than the shared receptor subunit.
Licensed (as Adtralza) for moderate-to-severe atopic dermatitis in adults and adolescents 12 years and older who are candidates for systemic therapy.Dosing: 600 mg subcutaneous loading dose, then 300 mg every 2 weeks. Same for adolescents.
Where it fits.
Generally less efficacious than dupilumab and slower to work, but many patients get there with time.
Symptoms of facial redness and eye symptoms tend to be less
Consider it where baseline ocular symptoms or facial eczema make dupilumab's adverse effects a particular concern
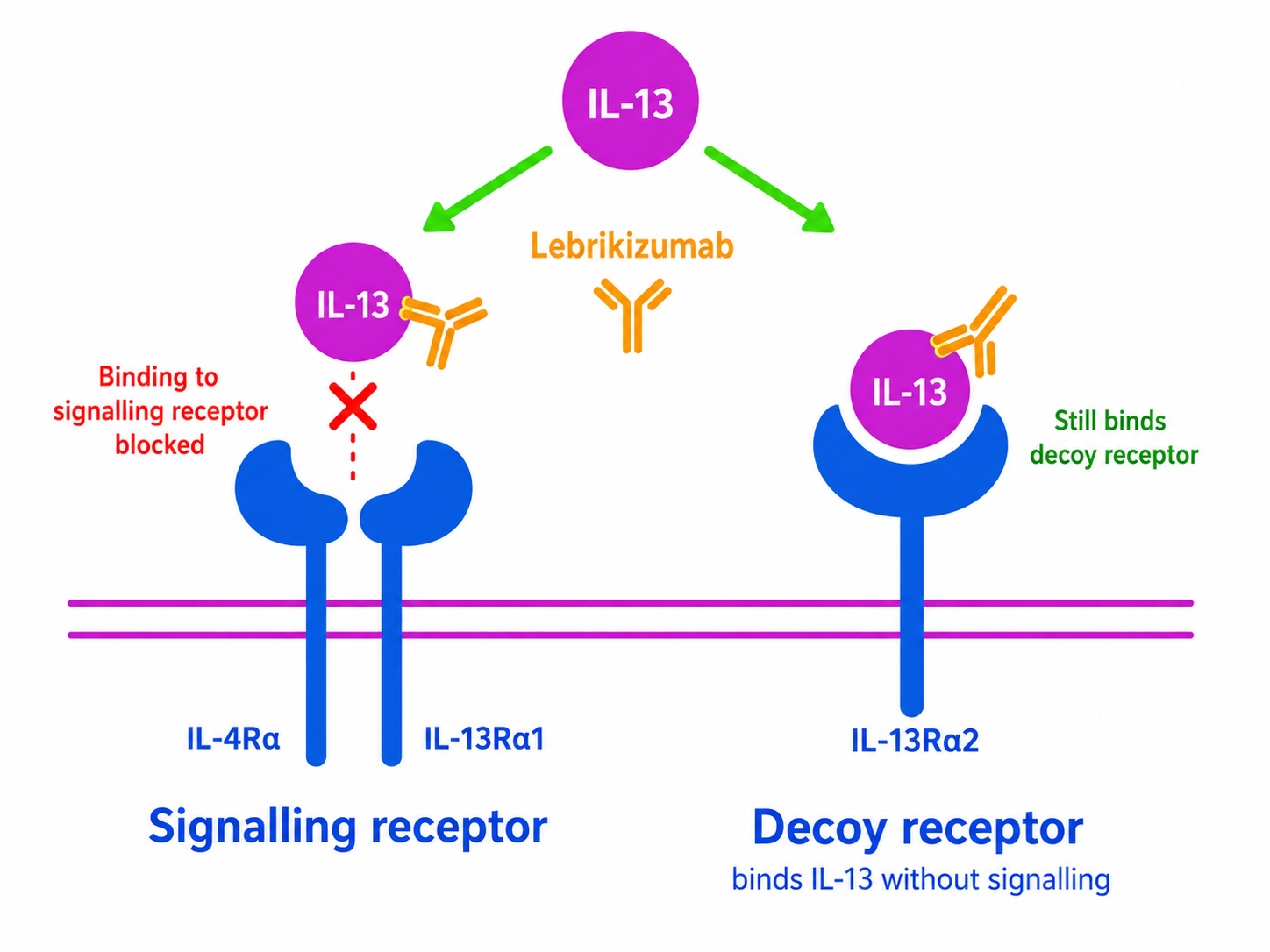
Lebrikizumab
It also targets IL 13 but in a different way to tralokinumab
IL-13 binds to 2 different types of receptors:
IL-4Rα/IL-13Rα1heterodimer is the signalling receptor
IL-13Rα2 is a decoy that binds IL-13 without triggering the inflammatory signalling.
Theoretically, tralokinumab prevents IL-13 from binding to both receptors.
Lebrikizumab selectively blocks IL-13 binding to the signaling receptor while preserving binding to the decoy receptor.
This may allow ongoing sequestration of IL-13 and theoretically to improve efficacy
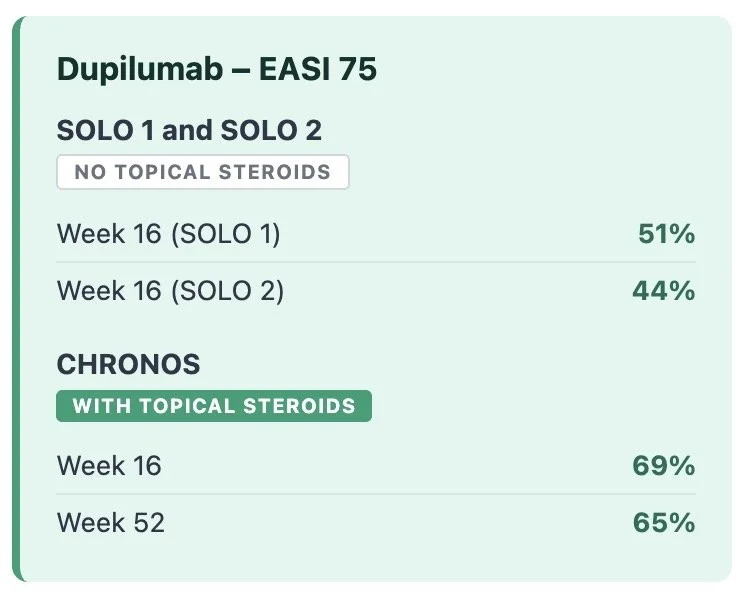
Lebrikizumab — efficacy
ADjoin is the long-term extension trial. Response appears stable out to two and three years rather than improving further.
Overall these trial results demonstrate comparable efficacy with dupilumab
Lebrikizumab side effects -
It has been hypothesized that lebrikizumab could carry a lower risk of conjunctivitis and facial erythema than dupilumab, but both events have been reported in lebrikizumab trials." "To date, evidence is insufficient to conclude that there is a meaningful reduction in these adverse effects.
Dupilumab, tralokinumab, lebrikizumab trial comparison
Nemolizumab
Humanised anti-IL-31 receptor α monoclonal antibody — blocks the function of IL-31, the cytokine that drives itch.
Mechanism:
IL-31 is an IL-6-family cytokine, signalling through a heterodimer receptor (IL31RA + OSMRβ)
Secreted mainly by Th2 cells, in parallel with the other atopic cytokines (IL-4, IL-13)
Receptor sits on peripheral sensory neurons, keratinocytes and various immune cells
Much more highly expressed in AD (and prurigo nodularis) than in healthy or psoriatic skin
IL-31 doesn't just cause itch — it also:
Recruits Th2 and other atopic cells to the skin
Acts as a neuronal growth factor (more itch neurons in the skin)
Drives structural change — epidermal hyperplasia and fibrosis
Licensed in the EU for:
Atopic dermatitis – Moderate-to-severe disease in adults and adolescents (≥12 years) who are candidates for systemic therapy.
Prurigo nodularis – Moderate-to-severe disease in adults who are candidates for systemic therapy.
Dosing
Atopic dermatitis: 60 mg subcutaneously at Week 0, then 30 mg every 4 weeks. If clear or almost clear after 16 weeks, maintenance may be reduced to 30 mg every 8 weeks.
Prurigo nodularis: 60 mg subcutaneously at Week 0, then:
<90 kg: 30 mg every 4 weeks
≥90 kg: 60 mg every 4 weeks
Efficacy - Atopic Eczema ARCADIA 1 and 2 (Silverberg et al., Lancet 2024)
Phase 3: ARCADIA 1 and 2
This could be a "slow-burn" drug — it appears improvement continues well past the 16-week readout. In Japanese long-term studies (Kabashima et al., Br J Dermatol 2022), EASI improvement deepened from around 45% at week 16 to roughly 78% by week 68 in those who remained on treatment, with itch scores falling in parallel. So someone who is technically a non-responder at 16 weeks (eg EASI-50 with a big DLQI improvement) may be much better by a year — so don't write it off too early if the trajectory is right.
Efficacy - Nodular prurigo Olympia 1 and 2 (Ständer et al. JAMA Dermatol. 2024)
Side effects
Reported in the trials
Nemolizumab was generally well tolerated across the ARCADIA and OLYMPIA programmes, with a profile close to placebo-plus-topicals and no clear infection signal — it behaves more as an immunomodulator than an immunosuppressant.
In contrast to the IL-4/13 agents, there has so far been no signal for conjunctivitis, head-and-neck dermatitis, musculoskeletal symptoms or psoriasiform switching.
The common events were headache, nasopharyngitis and URTIs, with urticaria and dermatitis in the SmPC.
Two signals stand out:
Peripheral oedema
Worsening of asthma (caution in significant asthma, even though it wasn't prominent in phase 3).
Observations from the St John's cohort
Early real-world experience has surfaced paradoxical skin reactions in a minority of patients.
Two patterns are seen: a desquamating, almost sunburn-like exfoliative dermatitis, sometimes with marked erythema; and a profound discoid (nummular) eczema, particularly in those with prurigo nodularis.
Peripheral and facial oedema also occurs, and it isn't always clear whether these represent a flare of the underlying eczema or a genuinely new drug-related rash. The reassuring message is that they are often manageable — many patients settle within a week on oral prednisolone and intensive topicals and can continue treatment through the reaction.
JAK inhibitors
Mechanism of action
There are only four members proteins of the JAK family:
Cytokine binding activates receptor-associated JAKs.
These phosphorylate the receptor and recruit STAT proteins, which are then phosphorylated, pair together and enter the nucleus to regulate gene expression.
JAK inhibitors block this intracellular signalling step, preventing multiple cytokine signals from reaching the nucleus.
The same JAKs are shared by multiple cytokines:
Different cytokine receptors recruit these JAKs in different combinations.
The important point is that the same JAKs are reused by many different cytokine receptors.
A JAK is therefore not linked to only one cytokine or one disease.
Simplified examples of overlapping JAK use by cytokines involved in atopic dermatitis. The same JAK family members are also used by many other cytokine receptors.
Why does this matter?
A biologic usually blocks one cytokine or one cytokine receptor.
A JAK inhibitor acts further downstream so blocking one JAK can reduce signalling from several cytokines at once
For instance, in atopic dermatitis, JAK1 is involved in:
IL-4 and IL-13 — type 2 inflammation and barrier dysfunction
IL-31 — itch
Other pathways involved in immune activation
This helps explain the rapid improvement in both eczema and itch with a JAK1 targeting JAKi
However, JAK signalling is also important for:
Antiviral and antimycobacterial defence
T-cell and natural-killer-cell function
Immune surveillance
Production of red cells, platelets and white cells
This promiscuous action explains both the efficacy and adverse effects of JAK inhibitors.
What do the different JAKs do?
JAK 1 - broad immune regulator
Important in both innate and adaptive immunity
Signals: interleukins (IL-2, IL-4, IL-6, IL-13, IL-15, IL-31) and interferons
Role: allergic responses (IL-4/IL-13/IL-31), acute inflammation (IL-6), antiviral defence (interferons)
Targeted in: atopic dermatitis (via IL-4/13), and other inflammatory disease eg IBD, RA
Issues: impaired antiviral and immune signalling — herpes simplex, herpes zoster, other infections, changes in lymphocyte and neutrophil counts. Reduced immune surveillance may also contribute to malignancy risk
JAK2 - the blood and growth kinase
Its most critical role is in haematopoiesis
Signals: erythropoietin (red cell production), thrombopoietin (platelet production), myeloid growth factors (neutrophils and granulocytes), growth hormone, prolactin
Role: signals bone marrow to make blood cells; also systemic growth and lactation
Targeted in: myeloproliferative disease
Issues: anaemia, neutropaenia and thrombocytopaenia
JAK3 - lymphocyte and NK cell function
The only JAK largely restricted to immune cells, and it only ever pairs with JAK1
Signals: IL-2, IL-4, IL-7, IL-9, IL-15, IL-21 — the common gamma chain cytokines
Role: development and function of T cells and NK cells
Targeted in: alopecia areata (ritlecitinib — JAK3 plus TEC family)
Issues: lymphopaenia, reduced NK cell function, viral infection including herpes zoster. Does not carry EPO or TPO signalling, so marrow suppression is less prominent than with JAK2 — but ritlecitinib still needs lymphocyte and platelet monitoring
TYK2 - innate immunity and IL-12/23 axis
Signals: IL-12, IL-23, type I interferons, IL-10 family
Role: Th1 and Th17 differentiation, antiviral defence, immune regulation
Targeted in: psoriasis and psoriatic arthritis (deucravacitinib)
Issues: appears milder — nasopharyngitis, URTI, herpes simplex, acne, folliculitis, mouth ulcers. No routine ongoing bloods, but TB and hepatitis screening before starting. Not subject to the EMA class restriction, though the label still carries the JAK class warnings as potential risks
Important caveat:
No JAK inhibitor is fully specific. All block more than one JAK to varying degrees (especially at higher doses).
So you cannot predict a drug's side effect profile from its primary target alone — assume some degree of class effect with any of them.
JAK inhibitors in atopic eczema:
JAKi used in atopic eczema can be considered selective (ie focus on JAK 1) or non-selective (ie focus on JAK 1 and 2)
| JAK 1 | JAK 2 | JAK 3 | TYK 2 | |
|---|---|---|---|---|
| Baricitinib | +++ | +++ | + | ++ |
| Abrocitinib | +++ | + | – | + |
| Upadacitinib | +++ | + | + | + |
Practical pharmacology:
All are oral tablets taken once daily
Two doses are given for each agent which gives more flexibility to use
Half life is very short - generally between 5 and 15 hours so can have tight control
Practically, that means it is mostly out of the system by 48 hours, and there is effectively complete washout in 3-5 days (x5 half lives)
This cuts both ways - it is useful if you need the drug gone quickly for infection, surgery or travel, but it also means a missed prescription leads to rapid relapse
Stop if don’t have adequate response by 16 weeks
Primarily renally cleared, but metabolised in the liver (consider drug interactions)
Adverse effects JAK inhibitors
Notable adverse events
The main concerns with JAK inhibitors are infection, malignancy and MACE (major adverse cardiovascular events) and VTE
These are real, but the evidence behind them is easily misread — worth knowing where it came from before you counsel anyone
The class warning:
EMA and MHRA issued a warning that applies to the whole class of JAKi
Increased risk of:
• Serious infection
• Malignancy
• MACE
• VTE
• All-cause mortality
...compared with TNF inhibitors
Use only if no suitable alternative in patients who are:
• Aged 65 or over
• Current or long-term ex-smokers
• At increased cardiovascular risk
• At increased cancer risk
Also: use with caution in any other VTE risk factor, and reduce the dose where possible in at-risk patients
Where the warning came from: ORAL Surveillance
Almost the entire class warning rests on one study
• Tofacitinib(a pan-JAK) vs TNF inhibitor
• Rheumatoid arthritis patients
• Over 50, with at least one cardiovascular risk factor
• >4,000 patients, median follow up 4 years
• Non-inferiority design —
The study set out to prove tofacitinib was "not worse than" the TNF inhibitor — and it couldn't prove that. It means the trial wasn't able to rule out a higher risk with confidence. So in essence it wasn’t able to demonstrate but instead couldn’t rule out harm.
The hazard ratio for MACE with tofacitnib 5mg bd vs TNFa is 1.24 — a modest relative increase, from a trial designed to detect exactly this kind of difference in a high-risk population
In absolute terms, this worked out to roughly 9 vs 7 MACE events per 1,000 patients per year — a difference of about 2 extra events per 1,000 patients, per year, in a population already selected for cardiovascular risk
Why it may not apply to our patients
Different population
RA is a different disease with different baseline cardiovascular risk
Deliberately enriched for risk: over 50, at least one CV risk factor
Many eczema patients we start a JAKi are young with no contraindications
Different drug
Tofacitinib is pan-JAK — the widest possible off-target profile
Not the JAK1-selective agents we use in eczema
Different comparator
Compared against a TNF inhibitor, not placebo
Some studies suggest TNF inhibitors may themselves be protective against malignancy
So this may be a neutral drug compared against a protective one, rather than a harmful drug compared against a neutral one
Wording of guidance also has grey areas?
• What counts as long-term smoking?
• How long after quitting does risk normalise?
• Does a previous BCC count as increased cancer risk?
What do we do?
No definite answers — need good clinical judgement, documented counselling and close follow up if have potential risk factors
Infection
This is the most consistent of the three risks, and the one you will actually see in clinic
Herpes simplex and herpes zoster:
The clearest infection signal with oral JAK inhibitors is an increased susceptibility to herpes-virus infection and reactivation.
Long-term pooled safety data for abrocitinib included 3,802 patients, representing more than 5,200 patient-years of exposure and treatment for up to almost four years. Simpson et al, Am J Clin Dermatol 2024
Herpes zoster occurred at:
2.1 cases per 100 patient-years with abrocitinib 100 mg
4.7 cases per 100 patient-years with abrocitinib 200 mg
For comparison, background rates are approximately 0.3–0.5 per 100 patient-years in the general population and 0.5–0.8 per 100 patient-years among people with atopic dermatitis.
The risk therefore appears several-fold higher with abrocitinib and is dose dependent
Most episodes were mild or moderate, cutaneous and limited to a single dermatome.
However, multidermatomal and serious infections occurred, including ophthalmic zoster, disseminated varicella-zoster infection and zoster meningitis.
The Greenbook in the UK now states that all patients over the age of 18 been given a JAKi should be given the Shingrix vaccine
Unfortunately, we don’t have an funding pathway for this in Ireland and patients need to source it privately through GP/pharmacy which can be expensive
Herpes simplex was also more frequent at the higher dose:
5.1 cases per 100 patient-years with abrocitinib 100 mg
7.7 cases per 100 patient-years with abrocitinib 200 mg
Most herpes-simplex infections were non-serious, although serious cases included eczema herpeticum and ophthalmic herpes simplex. Interestingly, eczema herpeticum was not dose dependent and was numerically less frequent with 200 mg, possibly because better eczema control improved the skin barrier.
Management of herpes simplex/zoster:
Quantify the risk before you start:
Risk is not uniform across patients, and the pre-treatment history is where most of the useful information sits.
Seek a history of:
Previous herpes zoster — how many episodes, which dermatome, any ophthalmic involvement
Recurrent or severe orolabial/genital HSV — frequency, whether previously on suppression
Previous eczema herpeticum, and how many episodes
Chickenpox history / previous varicella vaccination
Immunosuppressive co-medication (systemic steroids, methotrexate, ciclosporin) — combinations amplify risk
Factors associated with higher infection risk on JAKi:
Extremes of age
Prior recurrent infection before starting
Higher dose
Lymphopenia
Practical implication:
If a patient has a strong herpes history, that doesn't automatically exclude a JAK inhibitor — but it should change three things: your dose choice, your vaccination plan, and whether you start antiviral prophylaxis on day one.
Zoster (Shingrix)
Shingrix is recombinant and non-live, so it is safe in immunosuppression — unlike the live Zostavax, which is contraindicated.
In Ireland NIAC recomends the vaccine in immunocompromised adults aged 50+, and should be considered at 18–49 in patients with immune-mediated inflammatory disease on immunosuppressive therapy explicitly listed
This issue is that it is not funded in Ireland and patients need to get this privately
Potential timing for vaccine (adapted from Guy’s and St. Thomas’ pathway)
Route B accepts a slightly blunted vaccine response in exchange for not leaving severe eczema untreated for three months.

Antiviral prophylaxis for HSV:
Not everyone needs it.
Consider in patients with a history of severe or frequent HSV before starting - eg eczema herpeticum or HSV near eyes
Prophylaxis pathway suggestion(adapted from St. Guy's and St Thomas' internal guideline):
If prophylaxis deemed necessary:
Week 0 — start JAKi and commence antiviral prophylaxis:
Aciclovir 400 mg PO QDS, or
Valaciclovir 500 mg PO BD
[doses for HSV suppression in immunosupressed patient]
Week 24 — review. Has the patient had an HSV recurrence despite prophylaxis, or is there other complexity in the history?
Yes → discuss with virology; individualised plan, may need ongoing or alternative cover
No → stop prophylaxis and switch to a "pill in the pocket" approach — the patient holds a supply and starts at the first prodromal symptom
The rationale for the 24-week limit is worth stating explicitly, because patients often want to stay on it: infectious diseases advice is that prolonged uninterrupted antiviral exposure carries its own risks, principally resistance.
Six months covers the early period of highest reactivation risk, after which most patients can be managed reactively.
Important caveat: if the patient has a history of HSV involving the eye, check with the treating ophthalmologist before stopping prophylaxis. Herpes simplex keratitis is one situation where indefinite suppression may be appropriate.
Treatment of breakthrough infection:
Other infections
Herpes is not the whole story.
Upper respiratory tract infection is the commonest adverse event of the class, and although most are trivial, the underlying pattern — more frequent and more severe viral and bacterial infection, pneumonia included — is characteristic of JAK inhibition.
Risk concentrates at the extremes of age and in patients with recurrent infection before starting.
Serious infection, meaning hospitalisation or death, is both dose-dependent and sharply age-dependent, rising in those over 65.
Risk of reactivation of hepatitis and TB so need to screen for them
In practice: screen properly, start older patients on the lower dose, and take a febrile illness in an older patient on a JAK inhibitor seriously.
MACE and VTE
The signal that generated the class warning, and the area where our eczema population differs most from the trial population
What ORAL Surveillance showed
MACE HR 1.33 for combined tofacitinib doses versus TNF inhibitor, 1.24 for 5 mg twice daily. Non-inferiority to TNF inhibitors was not demonstrated
In absolute terms from this study: roughly 0.9–1.1 versus 0.7 events per 100 patient-years
About 567 patients treated for a year to cause one additional MACE from this study
Pulmonary embolism was the earlier signal: in 2019 the data monitoring committee moved patients from 10 mg to 5 mg twice daily after higher rates of PE and death, so the VTE risk appears dose-dependent
Risk was concentrated in patients aged 65 or over who had ever smoked. In patients under 65 who had never smoked the MACE hazard ratios fell to roughly 0.9–1.1 — essentially no signal (Kristensen et al, Ann Rheum Dis 2023)
In dermatology populations the signal is not reproduced
Ingrassia et al, JAMA Dermatol 2024 — 35 RCTs of JAK inhibitors for dermatological indications, 20,651 patients, mean age 38.5 years
No increase in composite MACE and all-cause mortality (OR 0.83, 95% CI 0.44–1.57) or VTE (OR 0.52, 0.26–1.04)
But mean follow-up was under five months, so this speaks to short-term risk only
The eczema-specific data
In the Simpson abrocitinib analysis, VTE showed a marked age split: 1.7 per 100 patient-years in the over-65s versus 0.1 in the under-65s
Bunick et al — upadacitinib over six years: MACE and VTE both ran at roughly 0.1–0.2 per 100 patient-years, with no accumulation over time
Not all the data agree. A global cohort study with three-year follow-up found increased pulmonary embolism and DVT in atopic dermatitis patients on JAK inhibitors compared with dupilumab or methotrexate (Kridin et al, J Eur Acad Dermatol Venereol 2025) — longer follow-up than the trial meta-analyses, and the strongest counterweight to them
What this means in clinic
MACE and VTE risk is very much linked to the patient’s risk factors: age, smoking, prior thrombosis, immobility, obesity and cardiovascular risk factors. A 28-year-old with eczema and none of these is deemed much lower risk
Combined hormonal contraception is an additive VTE risk that is easy to overlook. Worth asking about before starting, and worth a conversation about lower-risk alternatives (eg IUD, implant)
In anyone prothrombotic, the signals from rheumatology are consistent enough to justify real caution — and if you proceed, use the lowest effective dose and counsel patient regarding the risk and things to look out for
Malignancy
Less consistent than the infection signal, and the numbers are smaller but important to consider the risks
What ORAL Surveillance showed
Malignancy HR approximately 1.5 versus TNF inhibitor
Driven mainly by lung cancer in smokers, with lymphoma and non-melanoma skin cancer also contributing
In absolute terms from this study: roughly 1.1 versus 0.8 cases per 100 patient-years.
About 276 patients treated for a year to cause one additional malignancy from this study
Remember this is a different population, different drug, different comparator compared to what we see in the eczema population
Against placebo and methotrexate the signal disappears
Russell et al, Ann Rheum Dis 2023— 62 RCTs and 16 long-term extension studies across six indications (RA, psoriatic arthritis, psoriasis, axial spondyloarthritis, IBD and atopic dermatitis), with malignancy as the primary outcome
Versus placebo or methotrexate: no increase in malignancy with JAK inhibitors
Versus TNF inhibitors: incidence higher — IRR 1.63 for all malignancies, 1.43 excluding NMSC. The gap between those two figures is itself an NMSC signal
Supports the idea that TNF inhibitors may be protective rather than JAK inhibitors harmful
The eczema-specific data are currently underpowered
Most JAK inhibitor eczema trials run only 12–16 weeks. A null result in a short trial with few events is not evidence of safety — it is evidence of insufficient follow-up. Cancer takes years to declare itself.
In the Simpson trial previously mentioned — abrocitinib, 3,802 patients, over 5,200 patient-years, up to four years of exposure
Malignancy rates were low overall but concentrated in older patients: malignancy excluding NMSC 2.4 per 100 patient-years in the over-65s versus 0.1 in the under-65s, NMSC 2.4 versus 0.2, and NMSC higher in current or former smokers
Bunick et al, J Eur Acad Dermatol Venereol 2026 — upadacitinib, over 9,000 patient-years, up to six years of exposure
Low malignancy rates throughout, with no sign of risk accumulating over time — the longest eczema-specific follow-up currently available (at time of writing)
NMSC is the exception —
ORAL Surveillance found non-melanoma skin cancer increased with tofacitinib compared with TNF inhibitors, and more so at the higher dose
The Russell meta-analysis points the same way: the excess versus TNF inhibitors was larger when NMSC was counted than when it was excluded
The abrocitinib long-term safety data show the same pattern inside an eczema population — NMSC clustered in patients over 65 and in current or former smokers, and was very rare in younger never-smokers
The extreme version of risk of NMSC with JAKi is seen with systemic ruxolitinib (JAK1/2) in haematology patients. In a matched cohort of patients with polycythaemia vera or myelofibrosis, ruxolitinib exposure carried an adjusted SCC hazard ratio of 3.24 - Lin et al, JAAD 2022
A separate UK case series of 90 such patients found these cancers behave aggressively — SCC outnumbering BCC, mostly poorly differentiated, SCC recurrence in nearly 60%, and metastatic NMSC the leading cause of death ahead of myelofibrosis progression (Rampotas et al, Blood 2024). That series had no comparator arm and is heavily confounded by the underlying malignancy and prior therapy, but the pattern of SCC is closer to organ transplant recipients than to the general population.
Bottom line
A real signal was seen for malignancy in one high-risk rheumatoid arthritis population, possibly amplified by the choice of comparator.
The dermatology datasets have not reproduced it for internal malignancy, but they are not yet powered or long enough to exclude a modest risk with long latency.
NMSC is different — risk does appear genuinely increased
Screening and monitoring
History/exam:
Consider risk factors: HSV, VZV, DVT, PE, Clotting family histor, CV risk factors or disease, smoking
Invesigations:
FBC
U&E
LFT
Lipids
CK
Hepatitis/HIV serology
TB screen: CXR/Quantiferon
Potential monitoring (with bloods at each appointment):
Nurse review 4 weeks (with bloods, particularly FBC)
Then review at 4 months - decide if to continue
Then 4 monthly x 1 year
Then 6 monthly
Barictinib
Targets JAK 1 and 2
Dose 2mg/4mg
Half life: 12.5 hours
4mg is best dose
BREEZE AD-1:
EASI 75 @ 16 weeks 24.8%
Adverse effects: 56% at 4mg
Serious adverse effects: 1.2%
BREEZE AD-4:
Combined Baricitinib/Topical corticosteroid vs Placebo/Topical corticosteroid
EASI 75 @ 16 weeks:
45% Baractinib Vs 20% Placebo
As targets JAK 2 also there is an increased risk of anaemia/thrombocytopaenia
Abrocitinib
Targets JAK 1
100mg/200mg
Half life: 5 hours
JADE study:
EASI 75 response rate 62.7% at week 12
EASI 90 response: 38.6%
200mg will be the licensed dose adults
100mg (in adolescents and people > 60 and people with decreased renal/hepatic function)
Works very quickly
JADE compare:
Abrocitinib vs dupliumab (all in combination with topical therapy)
Abro 200mg best: EASI 75 70.3%
Abro 100mg: EASI 75 58.7%
Dupilumab: EASI 75 58.1%
Placebo: 27.1%
Upadacitinib
Targets JAK 1
15mg/30mg
Half life: 8-14 hours
30mg adults
15mg adolescents
Will be licensed for people from 12 years of age
At 16 weeks:
EASI 75 of 72-79%
EASI 90 also very good
RCT comparing Upadacitinib vs Dupilumab
(Blauvelt et al, JAMA Dermatol, 2021)
N=924
EASI 75 week 16: Upadacitinib 71% vs Dupilumab 61%
But there was increased risk of significant infection in upadacitinib group
Monotherapy trial results summary
Lack of comparison trials currently so can’t make definitive conclusions as different studies had different methods etc
Below is results of EASI 75 at 12-16 weeks for the big monotherapy clinical trials for each agent
MISCELLANEOUS TOPICS:
ECZEMA, BACTERIA AND MRSA
The skin microbiome is complex and diverse
There is a wide variety of microrganisms (including fungi, viruses and bacteria)
It differs from anatomic site to anatomic site and this can be seen as early as day 2 in life
(eg infants delivered vaginally have microbiome rich in lactobacilli, if born by CS it is initially riched in organisms colonising mother’s skin)
The microbiome changes over time in response to may things (eg pets, rural environment)
The microbiome is very diverse in normal skin and also diverse in quiescent atopic skin.
Eczema disease severity correlates with reduced diversity and Staph aureus colonisatoin
Atopic dermatitis patients tend to be colonised with staph aureus more often then control population
Staph aureus colonised 30-100% of atopic dermatiits patients
Lesional skin > non-lesional skin and nose
Colonisation:
Increases risk of infection
S aureus toxins can act as superantigens activating lymphocytes and macrophages
S aureus can trigger multiple other aspects of the immune system, eg:
Initiating prodcution of TSLP which triggers a switch to Th2 skewing
S aureus may displace normal flora of skin (eg s epidermis)
Normal flora produce substances that decrease inflammation.
So overpopulating skin with pathogenic staph you lose a mechanism to suppress inflammation
MRSA:
11-34% of AD patients colonised with S aureus have MRSA
MRSA colonisation is associated with:
Eczema severity
Hospitalisatoin
Use of TCI and TCS
Having a healthcare worker at hom
Oral antibiotic therapy
If have an eczema patient who is very resistant to treatment you can swab skin to make sure they don’t have MRSA
MRSA carriage eradication:
1/Mupirocin in nares tds for five consecutive days
2/An appropriate wash (eg octenisan) daily x 7 days
To treat or not to treat Staph aureus colonisation:
For:
Colinisation with toxin secreating S aureus can contriute to pruritus and inflammation
Coloinsation is a risk for infection
Against:
S aureus is a common commensal
Eradication is difficult
Cochrane systematic review showed no clear evidence of benefit (although studies were small)
PVL TOXIN
PVL (Panton valentine leuckocidin) staph aureus:
PVL is a toxin produced by certain types of S aureus
The toxin can kill white blood cells and cause damage to skin and deeper tissues
Clinically it can present with cellulitis, abscesses, boils and folliculitis so suspect in eczema patient who is getting recurrent boils
Risk factors for PVL (5 Cs):
Close contact (eg contact sports such as rugby)
Cuts and grazes
Contaminated items (eg touching contaminated gym equipment, towels, razors)
Crowding (eg living in military accomodation, prisons, boarding schools)
Cleanliness (an unclean environment encourages the bacteria to spread)
Clinically it can present with cellulitis, abscesses, boils and folliculitis so suspect in eczema patient who is getting recurrent boils
To diagnose take a standard bacterial swab and make sure you state on the form that you would like them to analyse for PVL toxin otherwise they won’t look for it
Management:
PVL carriage should be treated with octenisan wash and nasal ointments similar to regimen for MRSA decolonisation
If have active skin and soft tissue infection look up local guidelines and/or discuss with microbiology:
For instance:
Abscesses can be incised and drained
If PVL + but not MRSA: Some regimens suggest Flucloxacillin
If PVL + and MRSA +ve: Some regimens suggest rifampicin and another antibiotic
Severe infections may require IV antibiotics
PVL related pneumonia can be a complication